Contents
User Tip: You can hover your move over the video bar to jump ahead to chapters within the video.
The Clinical Profile is the left-hand panel that appears in every patient's chart. It is home to important patient details including their allergies, problems, history and medications. The Clinical Profile is also used for documenting vaccines, growth charts and storing legal and confidential notes.
The Clinical Profile is always accessible when navigating the patient’s chart and can be edited by any user. It is designed to support seamless collaboration and documentation as you move through your patient workflows. Keeping the Clinical Profile accurate and up to date will allow you to make informed healthcare recommendations. You can even reference data from the Clinical Profile into notes and visit notes to facilitate documentation.
You can easily share the clinical profile by clicking on the "Print/Fax" button at the top to print the clinical profile or fax it to a collaborating provider.
If you use Elation's
Passport for Patients feature, you can even share the patient's clinical profile with them by choosing the related sharing preference.
Any record in the clinical profile can be referenced into a note or visit note to facilitate documentation of a clinical encounter. You can click the "Actions" button next to any header to export the entire section to a note or visit note. You can also click "Actions" next to a specific record to only export that record to a note or visit note.
Certain visit note formats also allow you to reference different sections of the Clinical Profile into your visit note with buttons directly within the visit note format itself. Review the various visit note formats in the
Visit Note Documentation Guide- Visit Note Formats article to choose the best format for your charting preferences.
Learn more about
using Clinical Profile documentation to facilitate charting here.
The Clinical Profile is designed to be efficient and supports the display of the SOGI (sexual orientation and gender identity) Patient Demographics fields. Preferred name (ex. full name if different from legal) and pronouns will display in the Clinical Profile if documented, while other important data, like the patient's insurance and contact details, remains easy to see and reference. Additionally, the Passport icon and hover tooltip now displays the patient’s current Passport activation or invitation status.
Underneath the demographics overview, you will see the next appointment date and time for the patient if one is scheduled and you will also see the date of the last documented visit (visit note) if there is one on file.
Utilize the Allergies section to document structured information about your patient's allergies. If no allergies are listed, default text of NKDA will be displayed in the Clinical Profile.
To document an allergy:
- Click the "+ Add Allergy" button in the Allergies section
- Fill in the following field as needed:
- Allergy= Use the drop-down menu to select the most accurate allergy information from Elation's database of allergens, ingredients and drugs. If you cannot find the substance in the database then type in your own text.
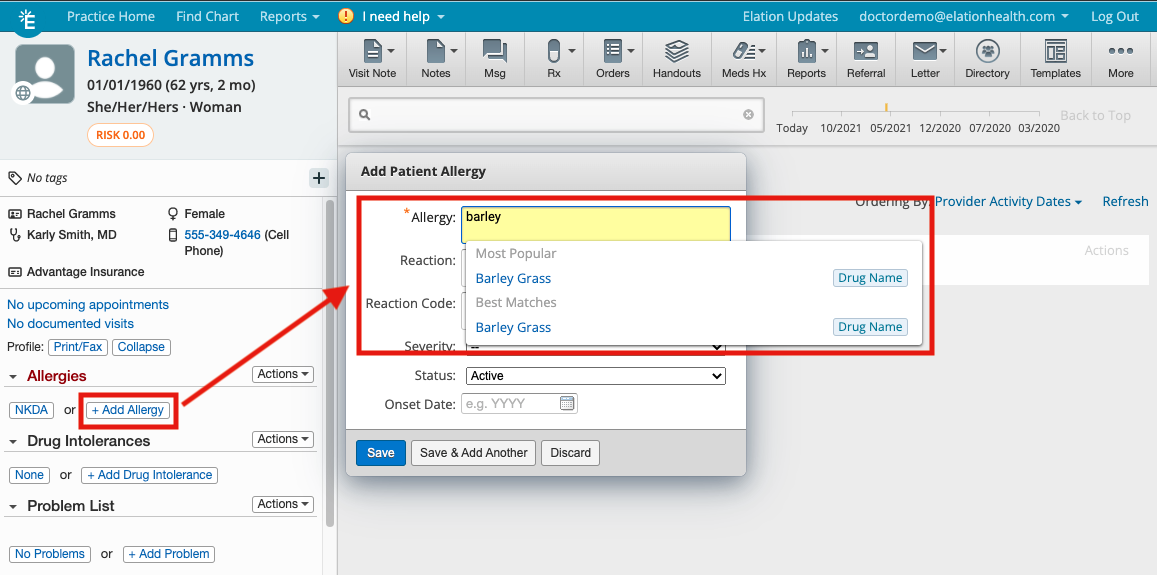
- Reaction= optional field that allows providers to enter structured data about the type of allergic reaction that occurs for the allergen, ingredient or drug listed.
- Reaction Code= optional field that allows you to enter a reaction code. The code is in the SNOMED-CT (Systematized Nomenclature of Medicine — Clinical Terms) format.
- SNOMED is a standardized, multilingual vocabulary of clinical terminology that is used by physicians and other health care providers for the electronic exchange of clinical health information. There is only a subset of SNOMED codes that apply to allergic reactions.
- Severity= optional field that gives everyone three options to select when documenting an allergy for a patient: mild, moderate and severe.
- Status= field that allows you to specify if the allergy is still active. The default is "Active"
- Onset Date= option field that allows you to note when an allergy began
- Click “Save” or “Save & Add Another” to save the allergy
You can edit any allergy documentation by clicking on the "Actions" button next to the documentation.
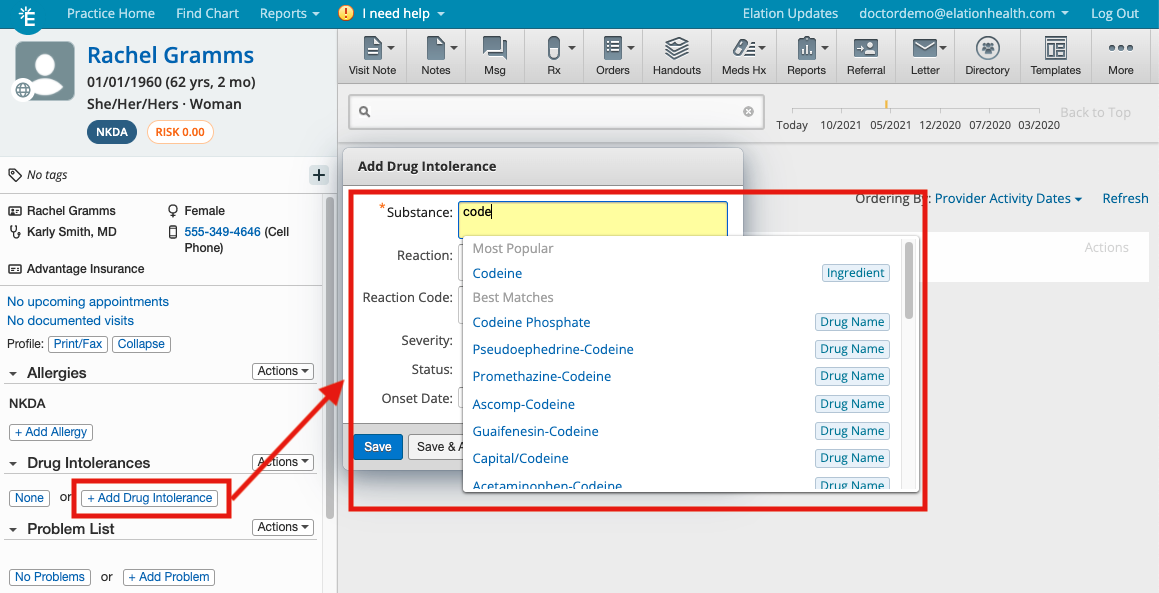
Use the Drug Intolerances section to document any drug intolerances that your patient has. If the patient does no have any, click "None" and the text No known drug intolerances will be appended to the Clinical Profile.
To document drug intolerances:
- Click "+ Add Drug Intolerance" in the Drug Intolerances section
- Fill in the following fields as needed
- Substance= Use the drop-down menu to select the most accurate drug intolerance information from Elation's database of drugs. If you cannot find the substance in the database then type in your own text.
-
User Tip: When you select from Elation's database, Elation will be able to use that information to detect potential drug reactions when you prescribe medications and notify you of interactions.
- Reaction= optional field that allows providers to enter structured data about the type of reaction that occurs for the drug listed.
- Reaction Code= optional field that allows you to enter a reaction code. The code is in the SNOMED-CT (Systematized Nomenclature of Medicine — Clinical Terms) format.
- SNOMED is a standardized, multilingual vocabulary of clinical terminology that is used by physicians and other health care providers for the electronic exchange of clinical health information. There is only a subset of SNOMED codes that apply to allergic reactions.
- Severity= optional field that gives everyone three options to select when documenting a drug intolerance for a patient: mild, moderate and severe.
- Status= field that allows you to specify if the drug intolerance is still active. The default is "Active"
- Onset Date= option field that allows you to note when a drug intolerance began
- Click “Save” or “Save & Add Another” to save the drug intolerance
Quickly see the problems, diagnoses and risk scores of the patient from the Problem List. This information is referred to as your diagnosis (Dx) when writing prescriptions, ordering labs and imaging for your patient. It also includes helpful risk score information that provides a snapshot into the severity of a patient's health risk.
To add a problem to the Problem List:
- Click "+ Add Problem" under the Problem List section
- Fill in the following fields:
- Search for a diagnosis= Use this field to search the diagnosis database for a diagnosis. You can search by ICD-9 Code, ICD-10 Code or description.
- Title= The Title will default to the description of the diagnosis you selected from the database but you can always adjust it to your preference.
- Dx Date= use this field to specify when the problem began. The date will default to 'today' if you do not change the date.
- Status= field that allows you to specify if the problem is active, controlled or resolved. The default is "Active"
- Synopsis= field that allows you to add notes about the diagnosis
- Click "Save" or "Save & Add Another" to save the Problem
Once saved, the problem can be edited or exported to your visit notes under several different sections by hovering your mouse over the problem, clicking on "Actions", then selecting the destination to export to.
Learn more about using the Problem List for other clinical workflows in the Problem List Guide.
The History section of the Clinical Profile is organized into distinct subsections to help you easily populate and reference details about your patient. Details within each section can be recorded in free-text or a structured manner.
- PMH (Past medical history)
- PSH (Past surgical history)
- FH (Family health history)
- SH (Social history)
- (Cognitive status)
- Func (Functional status)
- Psych (Psychological status)
- Habits
- Diet
- Exc (Exercise)
Free-text fields are fully customizable and allow you to personalize how you document details for the patient.
- Click on the text-field in which you’d like to add information. The field will turn yellow.
- Type the details for your patient and press the “Enter” key on your keyboard to save.
- If you’d like to revise text that has already been saved, click directly on the text and the field will turn yellow again to allow for edits.
- If you’d like to rearrange the order of your free-text fields, click on the 3 horizontal lines to the left of the text, hold down the cursor and drag the text and drop it in the appropriate order.
Structured text fields include a short pick-list of possible responses to a question. Examples include Social History (SH), Psychological Status (Psych), Habits and Exercise (Exc).
-
To add a structured question, click on the “add...” button to the right of the section heading and select an option
-
A new field or form will appear as a new line-item in the section. Click on the new field or the "Fill out form" button to proceed. See the Questionnaires section of this article for more information about structured screening forms.
-
To change the response, click on the dropdown arrow again and select a different option.
Elation’s built-in questionnaires allow you to easily document responses and calculate the score for common screenings. Please reference the Clinical Profile Guide- Structured Questionnaires for more information on how to best use this feature.
Your patient's current medications and medication history is an essential part of their clinical care. You can document medications to ensure your patient’s medications are up to date. Any permanent medications you prescribe or order will immediately be recorded in the Permanent Rx Meds or Permanent OTC Meds sections and a copy of any script that was prescribed during the last 6 clinical encounters will be available in Scripts Since Last 6 Visits.
New patients joining your practice may already be taking medications prescribed by other providers. To document an existing medication that a patient is actively taking (not order new medications):
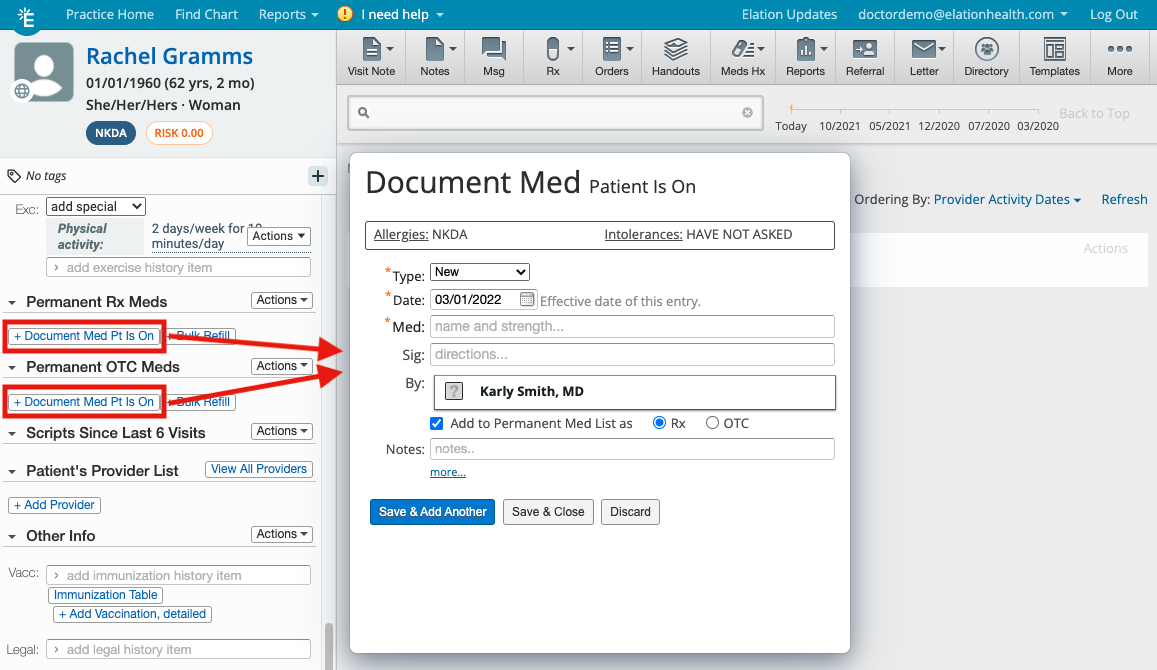
- Click “+Document Med Pt Is On” to open the dialogue box.
- Select “New”, “Change” or “Refill” from the Type menu and enter in the date the patient started the medication.
- In the Date: field, document the date the medication was started
- Enter the medication name in the Med: field by typing in the drug name and selecting it from the medication database
- Fill in the Sig field to note directions for use of the medication
- In the By: field, note the name of the provider that prescribed the medication for the patient
- Check off the "Add to Permanent Med List as" box to specify if you want to add the medication to the permanent Rx or OTC medications list. By default, Elation will automatically select to add the medication to the Permanent Rx Meds List
- In the Note field you can note any additional details about this medication as needed.
- Click the “more…” button at the bottom of the box to log the quantity of the medication, units and refills.
-
User Tip: Entering this information when you document new medications for patients is useful to make medication refills easy.
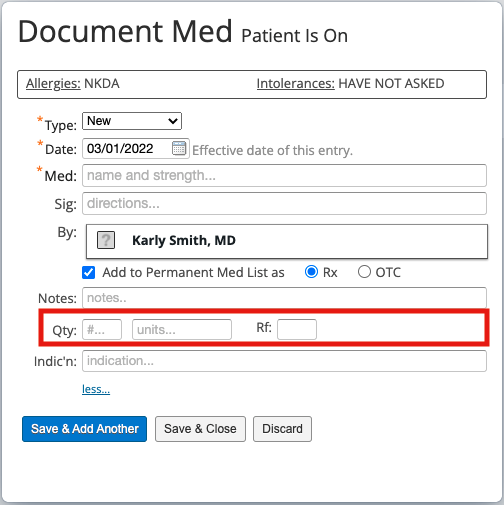
- Click "Save & Add Another" to continue documenting additional medications, or "Save & Close" when you are finished.
To view a full Medication History for the patient that includes temporary and discontinued medications, click the “Meds Hx” icon at the top of the patient's chart and click "Medication History". To learn more about managing the patient's medication list, review our Medication List Management Guide.
The
Patient's Provider List section allows you to see other providers who are collaborating with you to care for this patient or providers whom you have noted as caring for the patient. If you
sent letters or referral to any provider, they will appear in this list. You can also click "+ Add Provider" to add more providers to this list.
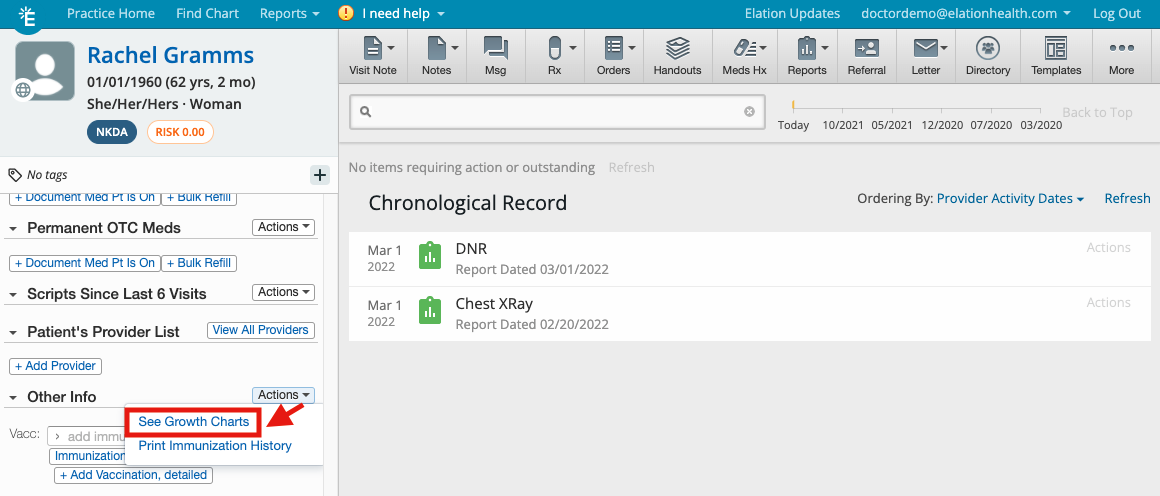
This section of the clinical profile is used to document vaccinations, file legal paperwork, and also where you will view growth charts for pediatric patients.
To view growth charts, click on the "Actions" dropdown to the right of the Other Info section, and click "See Growth Charts". Learn more about Growth Chart in the Growth Charts for Pediatric Patients article.
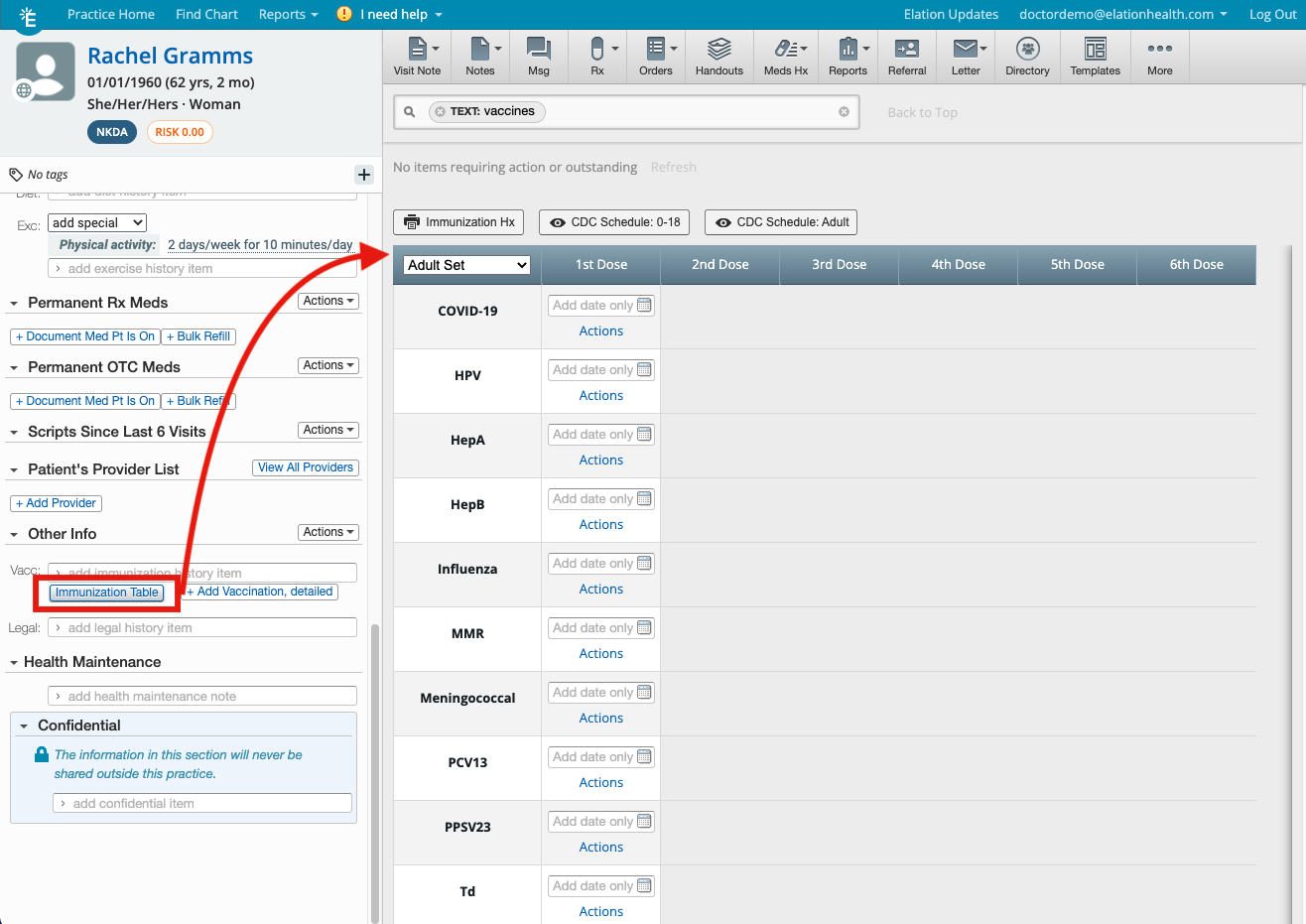
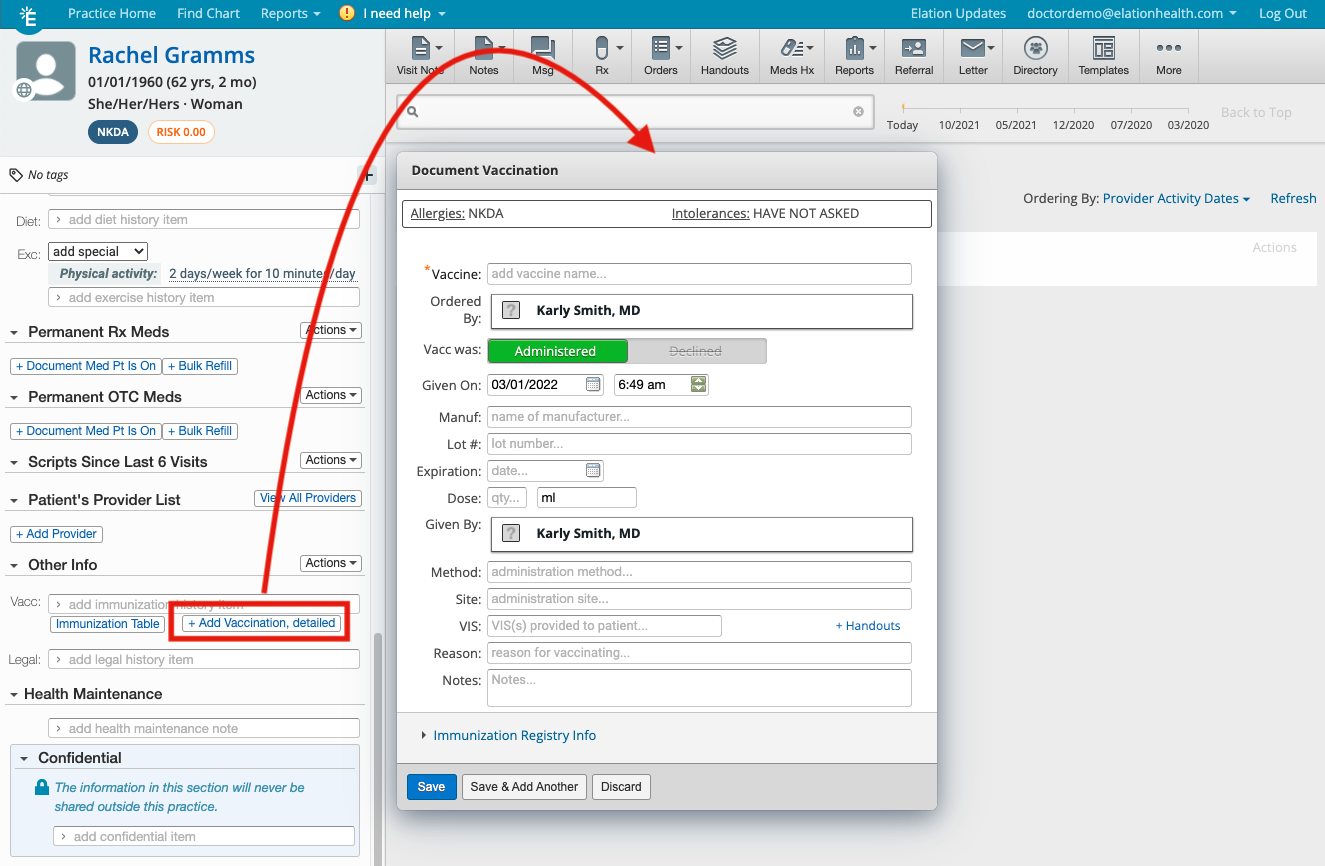
The Vacc: section allows you to record free-text or structure vaccination information. You can also click "Immunization Table" to view the Immunization Table for the patient or click "Actions" >> "Print Immunization History" under the Other Info header to print the patient's immunization history. Learn more about this section using the Vaccination Documentation Guide.
The
Legal section will allow you to document legal notes for the patient as well as reference legal documents in their chart. For legal documents, you can use the
drag & drop feature to file legal documents into the patient's chart under the
Legal Reports category and those documents will appear in this section of the Clinical Profile. This is useful for documents such as Release Forms, Patient ID Cards (Drivers License, Passports), Intake Forms or any other legal documents. You are also able to add a Document Tag to these forms to make it easy to identify who has or does not have specific legal forms on file.
The Health Maintenance serves as a central location for tracking and documenting current and outstanding health measures, such as exams and screenings. You can document the progress of health measures as free text or use Elation's structured Health Maintenance features. Learn more about this section in the
Health Maintenance Documentation & Reminders Guide.
The C
onfidential section of the Clinical Profile will allow you to document confidential and private notes for the patient that can only be seen by members of your office. Notes in the
Confidential section will never be printed or shared outside of your practice. Learn more about confidential records in the
Patient Chart Guide- Managing confidential records article.
Can I re-order the different sections of the Clinical Profile?
You cannot re-order the different sections of the Clinical Profile. They are outlined to match the layout of the different
Visit Note Formats we have available for users.
Can the problem list be ordered by relevancy not chronologically?
You can order your problems any way you like. The most recently added item is usually added to the bottom of the list. Use the 3 horizontal line button next to the problem to drag and reorder the list.
Can I re-order the different records in each section?
Yes, any
free-text field can be re-ordered. Use the 3 horizontal line button next to the record to drag and reorder the list.
Can I remove or hide specific sections of the Clinical Profile that I do not use?
You cannot hide or remove specific sections of the Clinical Profile but you can collapse all the sections by clicking the "Collapse" button above the Allergies section and then expand the sections you want to see to make the Clinical Profile more consolidated. Once you click "Expand" or reload the chart, all sections will be expanded again.
Can I make the entire Clinical Profile confidential?
You cannot specifically make the Clinical Profile confidential but you can make the entire chart into a
VIP Chart.
Learn about the VIP patient charts feature here.
Which parts of the Clinical Profile can patients see in Passport?
If you choose the
Entire Clinical Profile except the Confidential section option for your
Passport Sharing preference, patients can see every section of the Clinical Profile except the
Confidential section. The default Passport Sharing preferences are a Provider User Setting. You can change this on a per patient level by clicking on the "Passport" button at the top of the patient's chart.
Next Step
Start documenting clinical information in your patient's clinical profile too streamline charting!
Related Articles

